
U.S. Senator Ron Johnson has consistently been the only member of the federal government who has dared to expose the crimes being committed by Big Pharma through the government COVID response.
In 2020 Senator Johnson held meetings in Washington D.C. exposing the criminal activities of Big Pharma and federal health agencies in suppressing early treatment options for COVID-19 that thousands of doctors were using with a near 100% success rate.
Here in 2021 Senator Johnson has held meetings with testimony showing how dangerous the COVID-19 vaccines have been, giving a voice to those who have suffered injuries or lost loved ones who died after the shots.
Senator Johnson held another meeting in Washington D.C. today, one that has been planned for many weeks, regarding COVID-19 mandatory vaccines.
Some of the top scientists and doctors in the world attended, as well as several people suffering COVID-19 vaccine injuries.
He also invited:
- CDC Director Dr. Rochelle Walensky
- Secretary of Defense Lloyd Austin
- Secretary of Labor Marty Walsh
- Secretary of Transportation Pete Buttigieg
- FDA Acting Commissioner Janet Woodcock
- HHS Secretary Xavier Becerra
- NIAID Director Dr. Anthony Fauci,
- NIH Director Dr. Francis Collins
- Johnson & Johnson CEO Alex Gorsky
- Moderna CEO Stéphane Bancel
- Pfizer CEO Albert Bourla
- BioNTech CEO U?ur ?ahin
But none of these invitees showed up. They are, of course, Big Pharma controlled mouthpieces who only appear in public with the pharma-owned corporate media where they know ahead of time what the questions will be, and the script for how to answer them.
The corporate media also did not show up to cover this truly historic event in Washington D.C. The Roundtable discussion was recorded and is over 3.5 hours long, and you can watch the entire event at Senator Ron Johnson’s Rumble channel.
We have separated out several of the testimonies from this event into shorter segments that can be viewed on our Rumble and Bitchute channels.
Senator Johnson started off the session by stating that those who dare to tell the truth about the COVID-19 shots in public pay a high price for doing so.
Senator Ron Johnson: There is no need for COVID-19 vaccine mandates. If the vaccine worked and stopped transmission, those vaccinated would have no fear of the unvaccinated. If the COVID-19 vaccine does not stop transmission, then mandating them is pointless.
Brianne Dressen was an Astra Zeneca clinical trial participant from Utah, and is co-founder of react19.org, a patient advocacy organization dedicated to increasing awareness of adverse events
Brianne Dressen:
“I feel like I am being electrocuted 24/7.”
She thought she was alone and an isolated case, but then found out there were “thousands of us” being denied medical care and recognition as vaccine injured.
They decided to take action when they saw that children were being targeted with these deadly shots. They contacted every single political entity possible to talk about injuries and deaths from these shots.
“If you have an elected representative, they’ve heard from us.”
The media would not cover their stories, because they were told not to make the vaccines look bad.
Dr. Linda Wastila is a professor and Parke-Davis Chair in Geriatric Pharmacotherapy in the Department of Pharmaceutical Health Services Research and director of research for the Peter Lamy Center for Drug Therapy and Aging.
For more than two decades, she has conducted research focusing on prescription drug policy, quality, and outcomes.
She received her Bachelor of Science in Pharmacy from the University of North Carolina at Chapel Hill, where she also completed a Master of Science in Public Health.
In 1993, she received her doctorate in health policy from Brandies University, where she served as a Pew Health Policy Fellow. From 1994-2001, she served as senior scientist at the Schneider Institute for Health Policy, and was a lecturer at the Harvard Medical School. (Source.)
In June Dr. Wastila and several of her colleagues submitted a petition to the FDA regarding the experimental COVID shots. They called themselves “CALM” – the “coalition advocating for adequately licensed medicines.”
They were against the FDA approving any of the EUA COVID-19 “vaccines” until certain safety questions were answered, especially in regards to children and pregnant women.
The FDA denied their petition.
So not only are these questions on safety not answered, the shots are now being mandated, with no data at all on long-term effects. “How could we possibly supply informed consent without this information?”
We are citizens who have done our civic duty, but when we suffer serious adverse effects, we’re left high and dry by the FDA, the CDC, the NIH and medical professionals.
We are scientists alarmed by the toxic environment in academia and scientific publishing.
We are military leaders concerned about vaccine safety in the armed services.
We are clinicians who want to treat patients harmed by the vaccines but whose practices are limited by our employers and professional boards.
And we are lawyers and patient advocates seeking help for our injured clients and their families.
We are the people you haven’t heard from.
And we have nothing, absolutely nothing to personally gain from being here. Indeed, we have everything to lose, including our jobs, our titles, our livelihoods.
But we don’t intend to go away until we see some real change.
Cody Flint is a commercial pilot from Cleveland, MS who accumulated 10,000 hours of flight time and was diagnosed with left and right perilymphatic fistula, Eustachian tube dysfunction, and elevated intracranial pressure following Pfizer COVID-19 vaccination.
He experienced side effects while flying, and “by the Grace of God” was able to get the plane back down on the ground before blacking out, something to this day he does not even remember doing.
He experienced swelling of the brain following the Pfizer shot. He went through multiple surgeries and lost nearly a year of his life with his family.
I don’t know if I will ever be able to fly a plane again.
His career is destroyed, and he had to use up all of his savings just to pay medical bills. He feels the government has abandoned him as they refuse to help, after assuring everyone the shots were “safe and effective.”
Lieutenant Colonel Theresa Long is a Brigade Surgeon for the 1st Aviation Brigade, Ft. Rucker, Alabama, US Army.
She is a board certified aerospace medicine specialist with a Masters in Public Health.
Senator Johnson has invited me here to make a statement to him regarding my opinion about the life-threatening side effects about the COVID-19 vaccine.
My opinion is formed from my medical education, training, and my first hand experience treating soldiers injured by the vaccine.
This statement is made as a protective communication under the Military Whistleblower Protection Act, Title 10, USC 10-34.
I believe the COVID vaccine is a greater threat to soliders’ health and military readiness than the virus itself.
Over 200,000 service members have rejected the vaccine, yet the military is pressing forward without regard to the damage to the morale and readiness to process these soldiers out.
We have never lost 200,000 soldiers on the battlefield in a few months. Taking soldiers out of uniform has the same impact on readiness as losing them on the battlefield.
We only lost 12 active duty soldiers to COVID, yet we’re going to risk the health of the entire fighting force on a vaccine we only had two months of safety data on?
Ernest Ramirez is a father from Austin, TX whose only son collapsed playing basketball and passed away from myocarditis following Pfizer vaccination.
“My government lied to me.”
Kyle Warner is a 29-year-old professional mountain bike racer and a two-time national champion from Boise, ID who was diagnosed with pericarditis following vaccination. His career is now over.
The drug companies need to be compensating us if they are going to be testing on us.
Doug Cameron is a farm operations manager from Idaho, who is permanently paralyzed following COVID-19 vaccination.
I told my wife I felt like I drank poison. My whole body felt different. I went to bed at 10:00 at night. I woke up at 2:00 in the morning paralyzed from the diaphragm down.
My life as I knew it was gone.
Suzanna Newell is a triathlete from Saint Paul, MN diagnosed with an autoimmune disease and reliant on a walker or cane to walk following COVID-19 vaccination.
I was previously a long distance biker and triathlete. I was valedictorian in my high school, and now I struggle to retrieve words.
It’s like I aged 40 years overnight.
Kellai Ann Rodriguez is a young mother from Tacoma, WA reliant on a walker and suffering seizures following COVID-19 vaccination.
I lost my ability to speak naturally. I have become unable to walk without a walker. I never know when or if the tremors will come or go.
I can no longer cook, clean, or even pick up and hold my baby for too long before my body begins to shake uncontrollably or thrown into excruciating amounts of pain.
Doctors in the ER have allegedly told her that her injuries are all in her head, and even tried to get her committed to a mental health ward by calling social services on her.
You can watch the entire presentation here.
Comment on this article at HealthImpactNews.com.
See Also:
Why I am Proud to Wear the “Anti-Vaxx” Label – History and Science Show Vaccines Have NEVER Been Safe nor Effective
BOMBSHELL: Video Emerges Where Fauci and Others Planned for a “Universal mRNA Flu Vaccine” Which Became the “COVID-19 mRNA Vaccine” Because People were not Afraid Enough of the Flu Virus
COVID-19 “Vaccine” Casualties List
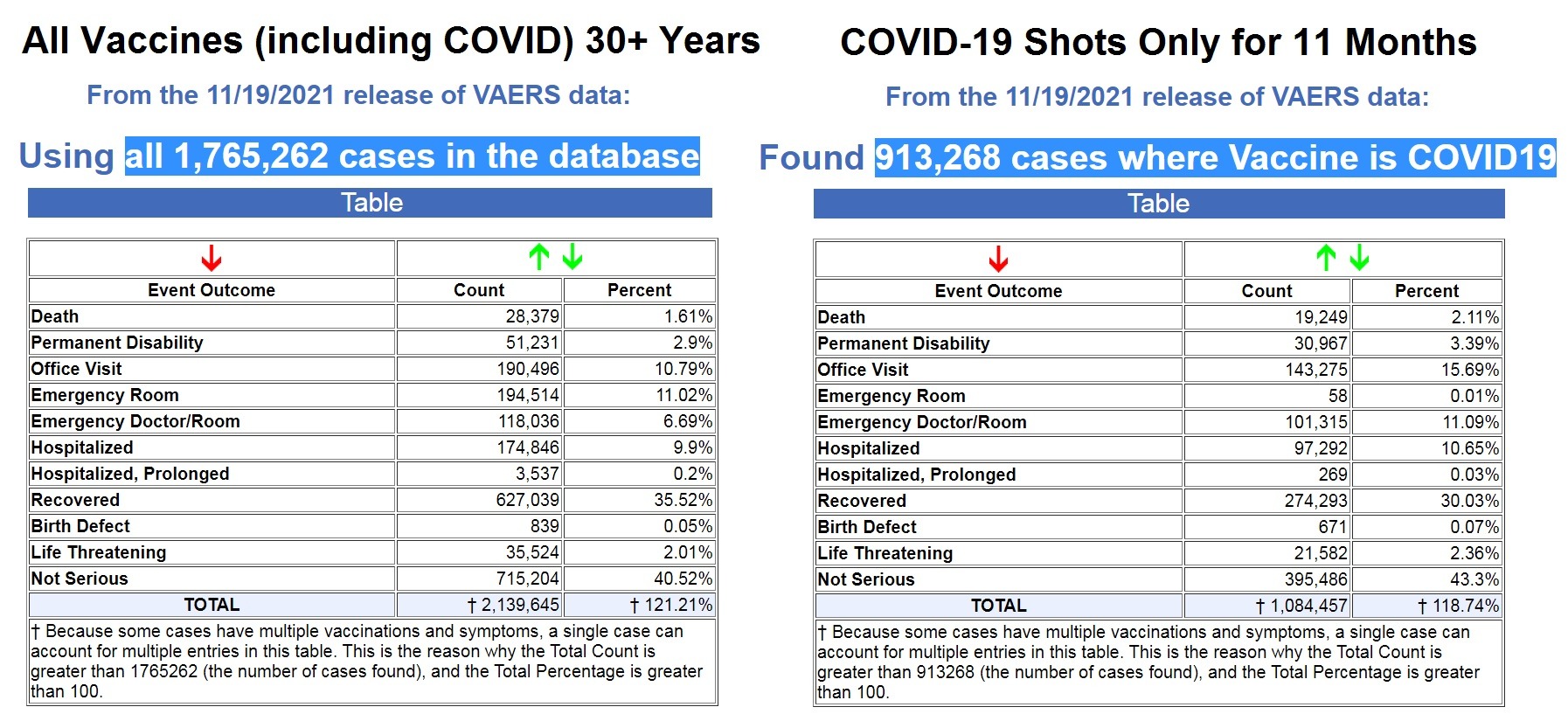
Vaccine Cult Exposed by Government’s Own Data: More than 50% of ALL Vaccine Adverse Reactions Reported for Past 30+ Years Have Occurred in Past 11 Months Following COVID-19 Shots
31,014 Deaths 2,890,600 Injuries Following COVID Shots in European Database of Adverse Reactions as Young, Previously Healthy People Continue to Die

Source: HNewsWire HNewsWire HNewsWire HNewsWire medicalkidnap
StevieRay HansenEditor,
HNewsWire.com
HNewsWire@protonmail.com
If it kills, it’s a pestilent. If you get sick and feel peony for a few days and lose your taste and smell, it’s a seasonal flu which we’ve had since the beginning of time, contrary to what phony doctors and or phony scientists have pushed as the gospel. Yes, it’s the gospel of evil, the gospel of Satan

![]()



Media Says Rise in Football Players Suddenly Collapsing is a “Coincidence”
The media has responded to the recent spate of high profile football players suddenly collapsing with heart problems in the middle of games by concluding that it is just a “coincidence.”